


A prosthetic limb can feel secure at first, then start to loosen as the body heals. Swelling reduces scar tissue firms, and the residual limb responds to walking, standing, stairs, and daily activity. These changes show up after the early fitting, when a person has already started using the limb more often.
That is why the preparatory vs definitive prosthesis plays a major role in recovery planning. The first device supports early mobility while the limb is still changing. The later prosthesis is planned once fit, skin response, balance, and movement are easier to assess.
This blog explains what changes, why socket fit shifts, and when another fitting may be needed.
What Changes During The First Few Months?
The first few months tell the prosthetist how your body responds to the new limb. During the first prosthetic fitting, short walking sessions may reveal socket movement, pressure areas, skin rubbing, or poor knee control. Amputation rehabilitation may begin between parallel bars before you move to crutches, a stick, or unaided walking.
Progress depends on healing, muscle strength, pain, age, and medical conditions. A Rehabilitation Council of India framework estimated 26.8 million persons with disabilities, including nearly 5.4 million with locomotor disabilities. Regular fitting reviews and gait training support a safer prosthetic care journey for many patients across India.
Preparatory vs Definitive Prosthesis: The Main Differences
The main difference is purpose. A preparatory limb helps you begin. A definitive limb supports longer use after the residual limb becomes more stable.
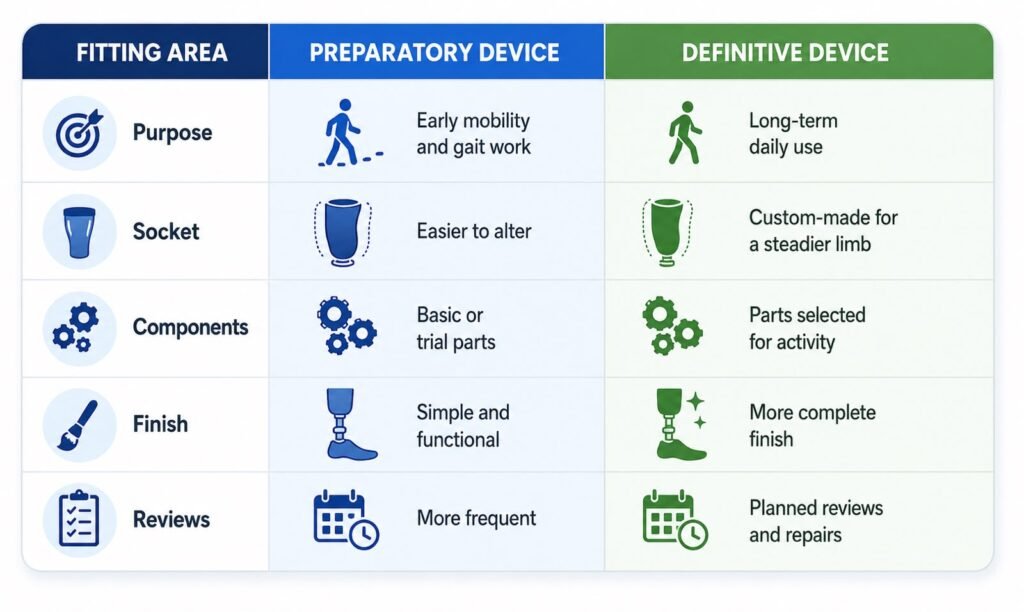
A temporary prosthetic limb may allow faster socket changes. The latter device usually follows when the residual limb has settled enough for a more refined fit.
Still, one timeline does not suit everyone. A young traumatic amputee may progress faster than an older patient with vascular disease.
How Socket Fit Changes As The Limb Settles
The socket controls most day-to-day comfort. Even an advanced knee or foot cannot rescue a poor fit.
After surgery, fluid leaves the tissues. Muscle bulk may be reduced. Scar tissue may soften. Because of this, the limb can become smaller over several weeks. You may notice the socket moving during stairs or longer walks.
Clinicians call this pistoning. At first, it may feel minor. After a few days, it can cause rubbing, redness, blisters, or skin damage.
During the preparatory vs. definitive prosthesis stage, the team may add prosthetic socks, pads, or liner changes. These are normal tools. Yet repeated sock additions often mean the socket needs a fuller review.
A patient may feel fine during a clinic walk but develop pain after commuting. Tell the prosthetist when pain starts, where it appears, and which task triggers it.
Why Component Choices May Change Later
Early components often support control and safety. Later choices can match pace, work, terrain, body weight, and personal goals.
For a lower-limb user, the team may review foot stiffness, shock absorption, knee stability, suspension, and overall weight. Someone who walks indoors needs a different setup from a person who climbs stairs and stands all day.
Upper-limb users also vary. Some need help with household tasks. Others want a work tool, body-powered hand, or myoelectric option.
An NIH-indexed review reported that bone-anchored prosthetic systems were associated with an 82%–90% increase in daily prosthesis use in studied patients. These systems need specialist screening and do not suit everyone.
The preparatory vs definitive prosthesis process gives the team time to see what you truly need. That is better than selecting advanced parts before your movement pattern is known.
How Walking Training Shapes The Final Prosthesis
Walking with an artificial limb is a learned movement. It takes repetition and correction.
During the early prosthetic care journey, a physiotherapist may work on weight transfer, balance, step length, turning, and stairs. Mirrors, floor markers, and parallel bars often help.
Small alignment changes can affect the whole body. A foot turned slightly outwards may disturb knee control. A socket set too high may alter hip movement.
This is why the first prosthetic fitting should act as a working trial. The team watches you move, then changes the setup where needed.
One patient may walk well on a clinic floor but struggle on a sloping road. Another may walk comfortably yet feel groin pressure while sitting. Both details shape the later design.
When The Early Limb Should Be Replaced
The switch does not depend on one fixed date. The body gives better clues.
A replacement may be considered when limb volume becomes steadier, skin remains healthy, gait improves, and the early socket needs repeated adjustment.
The preparatory vs definitive prosthesis discussion should cover work, travel, home layout, footwear, stairs, sitting time, and future goals. A shop worker who stands all day needs a different setup from an office worker.
A temporary prosthetic limb may remain useful while healing continues. A permanent prosthetic limb becomes more suitable once the clinical picture changes less often.
Before fabrication, the prosthetist may take a cast or digital scan. A test socket can reveal pressure areas before the final material is used.
What Changes In The Definitive Stage?
A definitive limb usually brings a more detailed socket, selected components, stronger finishing, and a design built around regular use.
It still needs maintenance. Liners wear out. Body weight changes. Components need servicing. The socket may need replacement later.
The final device should match ordinary life. Can you sit through a long journey? Can you manage wet floors? Can you wear work shoes? Can you stand long enough to cook or commute?
These questions are more useful than asking for the “best” prosthesis. The right device must suit your body, activity, and care plan.
How KARE Supports The Move To Long-Term Use
KARE supports patients through consultation, socket planning, trial fitting, gait work, counseling, and later reviews. The same clinical team can remain involved across each stage.
Our care includes one-to-one assessment, custom socket design, test sockets, alignment checks, and component selection. KARE also uses computer-aided design and fabrication methods, with microprocessor options where clinically suitable.
Patients can access physiotherapy guidance, balance work, weight transfer training, and walking practice. International-quality materials and components form part of the available choices.
KARE has centres in Bengaluru, Chennai, Mysuru, Kochi, Kolkata, Hyderabad, Thiruvalla, Durgapur, and Kozhikode. EMI options may help some families plan selected artificial limbs. The focus stays on fit, function, medical status, activity, and follow-up, rather than giving every patient the same device.
Conclusion
The first few months can change the residual limb, socket fit, and walking pattern. A staged fitting plan allows those changes to settle before long-term decisions are made.
The preparatory vs. definitive prosthesis process lets the team test fit, study movement, and choose a more suitable long-term solution. Speak with our team for assessment, fitting, gait support, and follow-up care. Start your next step with KARE, and let us plan it with you.
Frequently Asked Questions
What is a preparatory prosthesis?
A preparatory prosthesis is an early adjustable limb used during healing, volume changes, mobility training, socket assessment, and initial walking after amputation surgery.
How is a definitive prosthesis different from a temporary prosthesis?
A definitive prosthesis uses a custom socket and selected parts for longer use after the residual limb becomes stable enough for final fabrication.
When can a patient move to a permanent prosthetic limb?
A patient may move after wound healing, stable limb volume, healthy skin, improved strength, safer walking, and approval from the treating clinical team.
Why does the residual limb change after amputation?
Swelling reduces, muscles alter, scar tissue settles, and daily prosthesis use changes pressure across the residual limb during the first several months.
How does rehabilitation help during the prosthetic journey?
Rehabilitation develops balance, strength, weight transfer, walking control, skin care habits, and safer prosthesis use during each stage of fitting and review.


